
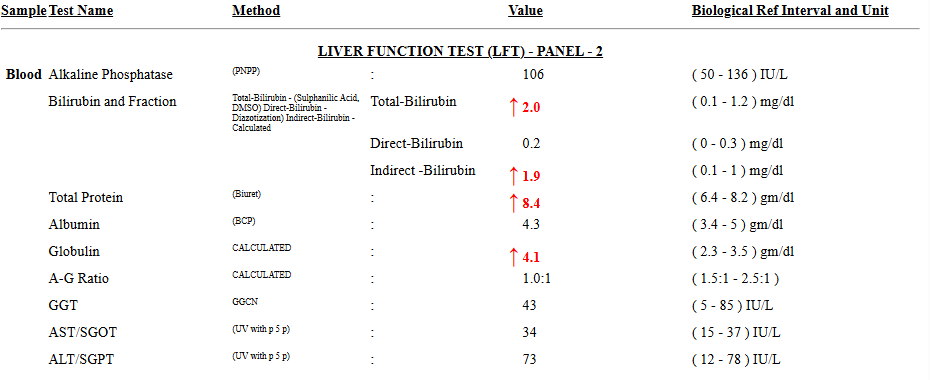
Have you encountered abnormal Liver function test with high indirect bilirubin? For example, total bilirubin is 2 mg/dL, and indirect bilirubin is 1.9 mg/dL. An isolated elevation of indirect (unconjugated) bilirubin is very common in clinical practice. The key is whether there is hemolysis vs impaired conjugation.
1. Most common & benign cause
➤ Gilbert syndrome
- Very common (up to 5–10% population)
- Mild elevation (usually <3 mg/dL)
- Normal LFTs (AST/ALT/ALP normal)
- Often fluctuates with:
- Fasting
- Stress
- Illness
- Dehydration
- No treatment required
👉 This is the most likely diagnosis if the patient is asymptomatic with normal labs.
2. Hemolysis (increased bilirubin production)
Causes:
- Hemolytic anemia
- Malaria
- Autoimmune hemolysis
- G6PD deficiency
Clues:
- ↑ LDH
- ↓ Haptoglobin
- ↑ Reticulocyte count
- Anemia
- Peripheral smear changes
3. Impaired conjugation (liver-related, non-hemolytic)
- Early liver disease (rare if other LFTs are normal)
- Drug-induced (e.g., rifampicin, atazanavir)
- Hypothyroidism (occasionally)
4. Rare inherited disorders
- Crigler–Najjar syndrome
- Severe, usually presents in infancy
- Not likely in adults with mild elevation
Practical Clinical Approach
Step 1: Check basic labs
- CBC
- Reticulocyte count
- LDH, haptoglobin
- LFT (AST/ALT/ALP)
Step 2: Interpret
- All normal (Normal Hb + normal retic + normal LDH + normal haptoglobin) → likely Gilbert syndrome
- Hemolysis markers positive (Anaemia + ↑ retic + ↑ LDH + ↓ haptoglobin) → evaluate hemolysis (CBC with peripheral smear, Reticulocyte count, LDH, Serum haptoglobin, Indirect bilirubin)
- Abnormal LFT → consider liver pathology
When to worry
- Total bilirubin >4–5 mg/dL
- Conjugated bilirubin rising
- Abnormal AST/ALT
- Symptoms: jaundice, dark urine, weight loss
Leave a Reply